
John Paul Gallardo, D.D.S., P.A., Periodontics and Implant Dentistry
From Our Office
to Yours….
Among the most significant technological advances in dentistry in recent years is cone beam computed tomography (CBCT). It’s use has grown exponentially, impacting almost every specialty. For many procedures, it is a great benefit in diagnosis and treatment planning.
CBCT is effectively used in dental implantology, endodontics, oral and maxillofacial surgery, orthodontics, and pathology assessment, because it provides horizontal, vertical, and axial views of structures.
CBCT is less expensive than traditional imaging, requires less space, has a limited field of view, has a shorter scanning time, and emits a lower average dose of radiation than CT scans.
This current issue of The PerioDontaLetter will review the latest applications of the dental CBCT in diagnosing and treating dental problems
As always, we welcome your comments and suggestions.
Cone Beam Computed Tomography
While two-dimensional (2D) radiography remains the imaging modality of choice in most dental practices, CBCT should be considered when the diagnosis cannot be adequately made with 2D imaging.
Despite advances in panoramic and intraoral imaging, these technologies still produce 2D images with inherent limitations, including magnification, distortion, and superimposition that can misrepresent structures.
Dental cone beam computed tomography (CBCT) produces three-dimensional (3D) images with accurate 1:1 measurements, while eliminating geometric distortion and superimposition. This, in turn, facilitates better diagnosis, treatment planning and follow-up care.
Although conventional medical computed tomography (CT) systems offer similar advantages — and provide information about soft tissue which CBCT does not — dental CBCT generates 3D data at a three to five times lower cost, with better spatial resolution (smaller pixels),

and with substantially lower absorbed doses of radiation. In addition, the larger size of conventional CT units makes them poor alternatives for dental offices.
CBCT uses a scanner specifically designed for imaging the head and neck, and additionally can produce 3D scans of the maxillofacial skeleton. The scanner is similar in size to that of a panoramic radiograph. But instead of a linear array of detectors, CBCT machines use a 2D planar sensor. X-rays are emitted as a large cone covering the area of the head being examined.
Since the cone beam irradiates a large volume area instead of a thin slice, the machine does not need to rotate as often as a CT scanner. It turns once, providing all the necessary information to reconstruct the region of interest (ROI).
This feature allows dentists to obtain 2D reconstructed images in all planes, and 3D reconstructions with minimal exposure to X-radiation.
The dental CBCT technology is specifically designed to produce highquality images of the teeth, jaws, and face by capturing tomographic images from different angles.
An X-ray tube and 2D sensor rotate around the patient’s head from 180 degrees to 360 degrees to gather imaging data. These images are then reconstructed into tomographic images with the aid of a computer.
CBCT in Detecting
Periodontal Defects
A complete periodontal assessment and a full-mouth radiographic series are still key components in establishing a periodontal diagnosis.
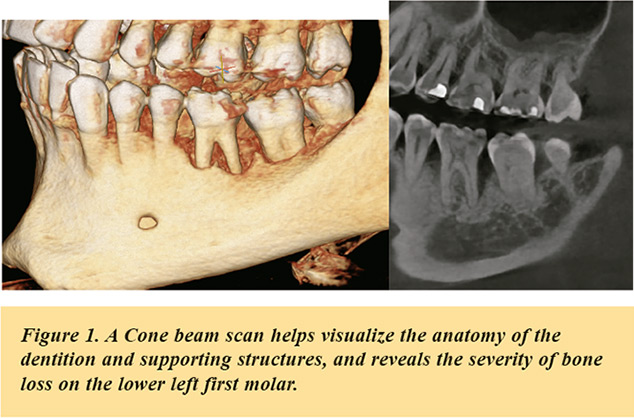
However, an exact measurement of the alveolar bone height and morphology using CBCT scans will enhance accuracy when assessing various periodontal conditions.
Cone-beam scans provide the ability to evaluate the morphology of periodontal defects, aiding in the diagnosis of their severity.
CBCT yields the highest sensitivity and greatest diagnostic accuracy for detecting periodontal defects.
Numerous studies have shown the increased accuracy of CBCT for detecting periodontal intrabony defects.
Grimard et al found 100 percent of all periodontal defects were detected with CBCT, while only 67% were detected with traditional radiography.
Vandenberghe et al showed that all bony craters and furcation defects were seen with CBCT, compared to only 56 to 71 percent of bony discrepancies visualized with conventional bite-wing and periapical films.
CBCT in Implantology
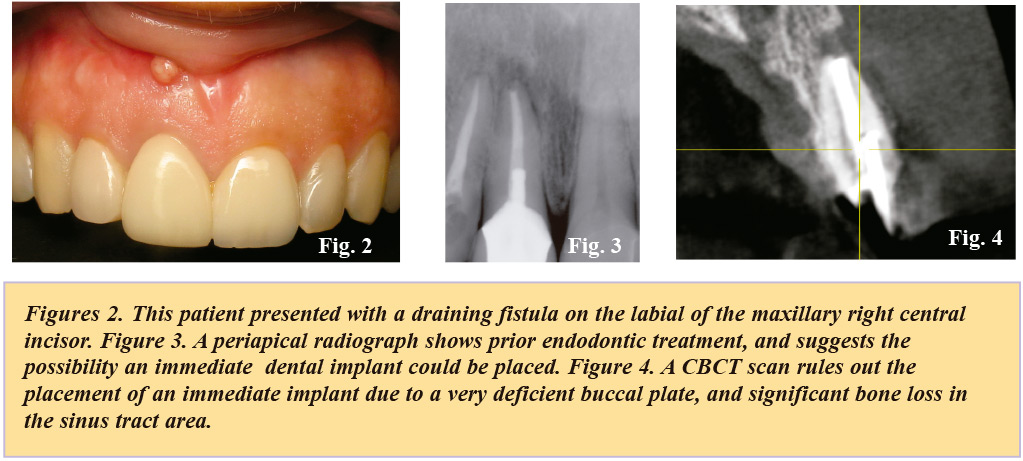
CBCT combined with the use of dedicated dental implant software has revolutionized the planning and placement of dental implants and is currently the imaging of choice when planning implant surgery.
CBCT offers a more accurate and safer positioning of dental implants, may reduce the time necessary for implant surgery, and often eliminates the need for open-flap surgery.
Furthermore, it facilitates a team approach to develop a more accurate, restoratively-driven treatment plan.
Dedicated computer software allows visualization and manipulation of the images of the patient’s jaw bone and surrounding tissue, making possible precise implant surgery.
Computer-generated surgical guides can be fabricated using CBCT scans and computer-aided manufacturing technology.
The implant surgeon can determine the implant type, size, and position within the bone, relationship to the planned restoration, and adjacent teeth or implants, including proximity to vital structures before surgery.
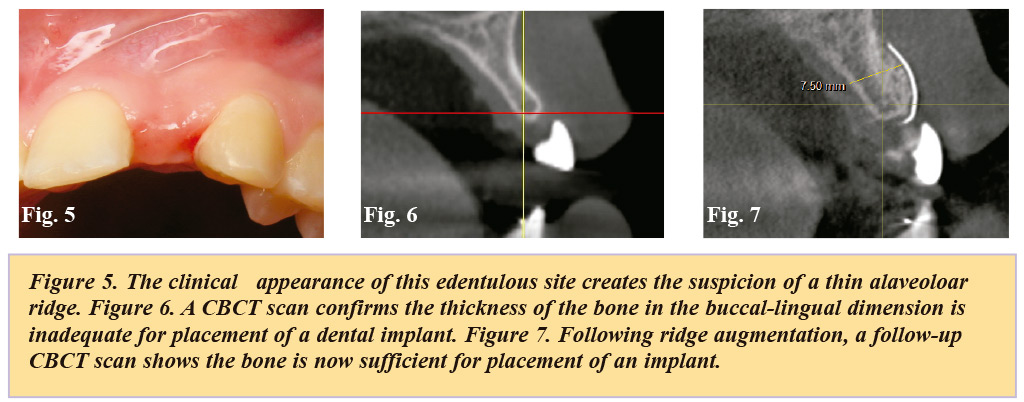
The quality images obtained by CBCT permit the implant surgeon to determine the height and width of available bone, soft-tissue thicknesses, proximity and root anatomy of adjacent teeth, and other vital structures.
The integration of CBCT with modern optical scanners could soon make conventional impression materials obsolete because of the ease of capturing surface features and occlusal morphology of teeth. To do this, a stone cast is scanned and transferred to a CBCT scanner with the same parameters as those used for the patient’s scan.
This facilitates the clinician’s ability to accurately visualize the patient’s anatomical structures, which in turn allows for minimally invasive surgery.
Maxillary Sinus
Floor Elevation
In the posterior maxilla, tooth replacement with dental implants often requires bony augmentation to increase the volume of bone at the floor of the sinus. If the amount of bone between the ridge crest and the maxillary sinus floor is inadequate — less than 5mm — a sinus augmentation procedure is indicated.
Preoperative CBCT or CT is recommended to accurately visualize structures within the antral space. These may include thickened sinus membranes, mucous retention cysts, septa, residual bone height, lateral wall bony thickness, and location of the arterial vessels traversing the lateral wall. This information is critical to safely perform sinus augmentation surgery.
CBCT in Oral and
Maxillofacial Surgery
Because CBCT eliminates the structural superimpositions seen in panoramic radiograph (PAN), it allows accurate measurement of surface distances, for example between the apices of the maxillary posterior teeth and the floor of the maxillary sinus.
This particular advantage has made CBCT the technique of choice for investigating, evaluating, and managing maxillofacial trauma.
CBCT is widely used in planning orthognathic surgery. Because CBCT software allows minimum visualization of soft tissue, oral surgeons can control post-treatment esthetics in cases of cleft palate and oral and maxillofacial defects.
CBCT is used routinely to detect oral and maxillofacial pathology. CBCT may help evaluate large odontogenic and non-odontogenic cysts and benign tumors of the jaws.
CBCT can show the extent of the lesion and the proximity to essential structures, such as the maxillary sinus. It may also help plan the therapeutic approach.
CBCT images are also used to determine bone structure and tooth orientation, assess impacted or supernumerary teeth, and the relationship of these teeth to vital structures.
It is used for pre and postsurgical assessment of bone graft recipient sites, and evaluation of jaw changes resulting from osteonecrosis.
CBCT is used to evaluate paranasal sinus pathology and/or defects; to locate the origin, location and extent of jaw pathology; and to detect, measure, and treat jaw tumors. Finally, it is used to evaluate patients with obstructive sleep apnea.
CBCT in Endodontics
CBCT imaging is useful for detecting, diagnosing and determining the appropriate treatment for many endodontic conditions.
Several studies have suggested that in diagnosing periapical lesions, CBCT images can be used to differentiate between apical granulomas and apical cysts.
CBCT is a reliable and far more accurate tool than 2D imaging to inspect and evaluate complex root canal anatomy and anatomical structures; assess and manage dentoalveolar trauma, and detect horizontal and vertical root fractures.
It measures the depth of dentin fracture, and evaluates external, internal, cervical and inflammatory root resorption — a diagnosis that is rarely possible when using conventional 2D radiographs.
CBCT measures the extent of a lesion, determines pulpal extensions, and the position and location of fractured instruments.
It assesses a tooth’s proximity to adjacent vital structures, which allows for accurate measurement of the size and extent of a lesion and the anatomy of the area.
And it evaluates endodontic complications like post perforation, detects periradicular bone changes that suggest root fractures, and offers presurgical review before endodontic therapy.
CBCT in Orthodontics
CBCT is a reliable tool for assessing the proximity of impacted teeth to vital structures that could inhibit orthodontic movement. With new orthodontic assessment software, orthodontists can use CBCT images for cephalometric analysis, making it the tool of choice for assessing facial growth, age, airway function, and tooth eruption disturbances.
When temporary anchorage devices (TADs) are used to enhance anchorage, CBCT provides visual guides for safe insertion, thus avoiding accidental, and perhaps irreparable damage, to roots.
CBCT may be indicated as part of orthodontic treatment planning when there are unerupted permanent maxillary canines, dilacerated teeth, unerupted or supernumerary teeth close to the inferior alveolar canal, and clefts that may require grafting.
CBCT for TMJ Disorders
Diagnostic imaging of the TMJ is crucial for proper diagnosis of joint disease and dysfunction. CBCT makes it possible to examine the joint space and the true position of the condyle within the fossa and alterations in the position of the disk.
CBCT’s accuracy and elimination of superimposition makes it possible to measure the roof of the glenoid fossa and visualize the location of the soft tissue around the TMJ, which can reduce the need for magnetic resonance imaging (MRI).
CBCT is the best imaging device for cases involving trauma, fibroosseous ankylosis, pain and condylar cortical erosion, and cysts.
Other CBCT
Applications
Dental and Facial Trauma: While intraoral radiographs may help in evaluating traumatic injuries, CBCT will be more likely to reveal root fractures, fractures of the alveolar bone, and displaced teeth.
Conclusion
CBCT imaging technology provides a clinical breakthrough, enhancing diagnosis, treatment planning, and more precise execution of complex dental procedures.
CBCT is critical for implant treatment planning. In all aspects of diagnosis, treatment planning, surgical preparation and execution, follow-up care, and management of complications, we can now treat our patients with increased precision and predictability.
The potential for further applications from dental procedure diagnostics to visual guidance is very promising.